
Premature Birth and Heart Disease
November 16, 2022 | Contributed by Dr L. Srinivas
17th November is designated as world Prematurity Day. Let us dedicate this day to understanding specific challenges involved in caring for the health of the tiny little premature babies, specifically related to heart disease in children.

A baby is said to be born premature or Preterm if he/she is born before completion of 37 weeks gestation. 5-18% of all deliveries globally happen to be preterm. Several physiological factors of development are lacking in a premature baby which ultimately decides the ultimate survival. Problems of prematurity with lung, intestine, kidneys, immune system and brain development amongst others put such babies at high risk. In a standard NICU set up with good intensive care doctors, nursing, infection control protocols, equipment and technical know how to handle complex ventilatory requirements the outcome of most babies has greatly improved. A Survival rate of more than 90% is now possible in babies who weight more than 1kg at birth. However, the presence of heart disease in children in this extremely vulnerable age group adds to the disease burden and makes management of such babies challenging for the treating medical team.
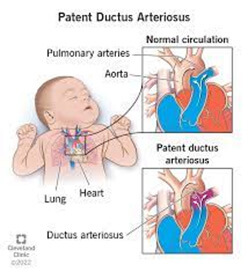
Patent ductus arteriosus (PDA) happens to be the most common confounding factor associated with the survival outcome. Nearly 50% of premature babies who weigh less than one kg at birth are known to have PDA. While most of the babies born with PDA can be managed with medications and ventilation support, surgery or device closure is indicated for those who cannot be managed with routine strategies. There are limited number of centers in India which have inhouse expertise in evaluation and interventional management of premature babies with PDA. With a good team approach comprising of Neonatologist, Pediatric cardiologist, Pediatric cardiac surgeon and nursing team outcome of such babies has greatly improved. Timely decision and intervention is the key for successful survival of such babies.
Another heart disease in children that is increasingly becoming common is the presence of persistent pulmonary hypertension in neonates. This problem is more common amongst borderline preterm babies. Due to complex interaction of lung maturity, meconium aspiration and lung vascular development, the pressure within the lung blood vessels could be persistently high and this condition is called primary pulmonary hypertension (PPHN). Management of PPHN in such vulnerable population of low birth weight is often challenging for the medical team. Again, the most common requirement for care of such babies is good intensive care and nursing team. Highly advanced mechanical ventilation strategies including high frequency oscillation ventilation and inhaled nitric oxide may be required occasionally. There is no role of cardiac surgery in this subset. Serial echocardiograms to monitor pulmonary artery pressure, heart function may be required to decide on response to treatment and its further modifications. For many children the cost of these procedures is extremely high. Organizations who work on congenital heart disease donations play a crucial role in helping these children survive by providing the required financial support.
Neonatal myocardium (heart muscle) also shows certain levels of immaturity in preterms. More often when such neonates are subjected to stress, myocardial dysfunction could be noted. Response to treatment is often unpredictable in such babies. It is extremely difficult to handle such babies with poor myocardial contractility who already are bothered by multiple factors affecting the premature babies. Constant monitoring of myocardial function, balance of fluids and inotropes are often required. Neonates who display severe myocardial dysfunction generally have poor outcomes.
There is no data to support that complex heart defects result in premature births or vice-versa. The presence of a complex heart disease in children that requires an open heart operation in a in premature baby is a night mare to any well accomplished team. Open heart surgery for correction of simple cardiac lesions may be possible for babies who weigh more than 1.8-2kg. Babies under this weight category generally do not have favorable outcomes. Most teams in the world do manage such babies medically with additional nutritional support in the hope to make the baby “grow” to an acceptable weight criterion. Again, many organizations which work in the area of congenital heart disease donations play a pivotal role in building awareness and providing financial support to those families who cannot afford this treatment.
At present we may have a reasonable understanding and protocols for managing premature babies with heart disease. Newer data and inventions in neonatal care are promising. Advances in biomedical technology, pharmacology, respiratory mechanics and skill development are the need of the hour for improved survival. In a resource limited country like India, provision of such advanced care for the non-affording is probably a bigger challenge. Cost effective strategies and facilities need to evolve. Charities and oragnisations helping in congenital heart disease donations continue to play an important role.
Dr L Srinivas is Consultant Pediatric Cardiologist at Jupiter Hospital, Thane