
Learning about the Transposition of Great Arteries
November 23, 2018 | Contributed by R Srivatsan
At Genesis Foundation, we get various referral cases of children that urgently require congenital heart disorder treatment and without it the plain truth is, they won’t live. A common malformation we have seen in many of the cases we get is Transposition of Great Arteries (TGA).
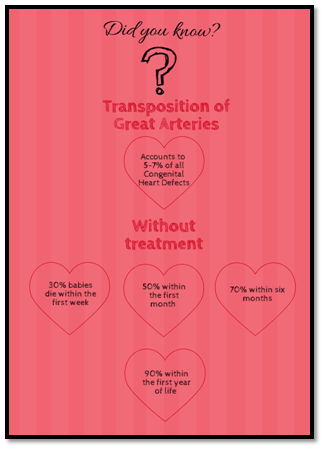
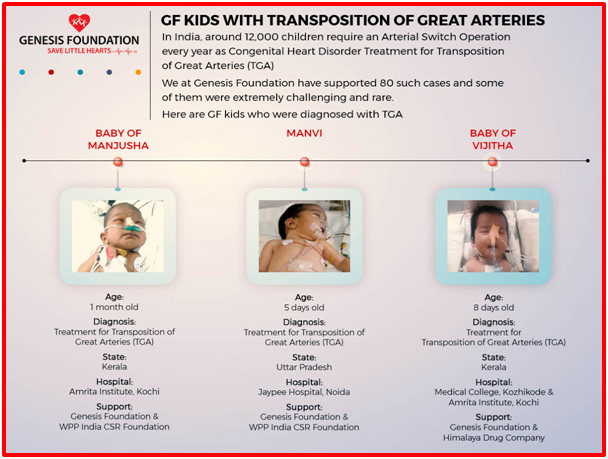
But, with advancements in medical sciences and in surgical interventions in the neonate can provide > 90% early and mid term survival and for many patients, a near to normal life. In India, around 12,000 children require an Arterial Switch Operation every year as Congenital Heart Disorder Treatment for Transposition of Great Arteries (TGA). However, only around 2000 such surgeries are performed.
We at Genesis Foundation have supported 80 such cases and some of them were extremely challenging and rare – where it was truly a matter between life and losing a child.
Anatomy
Doctors have chosen a variety of terms to describe the basic anatomic abnormality in TGA: the aorta arising from a morphologically right ventricle and the pulmonary artery arising from a morphologically left ventricle. The great arteries may be related normally or abnormally to each other, to the ventricles, to the ventricular septum, and to the AV valves. Normally and abnormally related great arteries customarily are designated in terms of their ventriculoarterial connections or alignments, that is, normal, transposed, double outlet right or left ventricle, and anatomically corrected malposition.
Coexisting Anomalies
Nearly half of the hearts with Transposition of Great Arteries (TGA) have no other anomaly except a persistent patent foramen ovale or a Patent Ductus Arteriosus (PDA). In the other half, isolated LVOTO with IVS is uncommon, about 5%. A Ventricular Septal Defect (VSD) is common and present in about 40% to 45%. These coexisting anomalies, together with AV valve and valve tensor abnormalities and aortic obstructive lesions constitute additional challenges for diagnosis and surgical interventions.
Other Associated Anomalies
Prior to the extensive present day use of prostaglandin E1 therapy, a PDA was found in almost half the neonates at the initial cardiac catheterization for BAS. The ductus is usually closed by 1 month of age.
Treatment
The immediate management of an infant with transposition focuses on establishing safe oxygen levels and stable cardiac and pulmonary function.
A continuous infusion of prostaglandin, a medication that will keep the ductus arteriosus open, is usually initiated when the diagnosis is suspected or confirmed. This will allow some mixing of oxygen-rich blood with oxygen-poor blood but may provide adequate mixing by itself.
A procedure called a “balloon atrial septostomy” is often performed once the diagnosis is confirmed. Before birth, all babies have a connection between the right atrium and the left atrium (called a foramen ovale). After birth, this normal connection may allow some mixing of blood to occur but may not provide enough mixing. The foramen ovale may be enlarged or stretched with a balloon, which will markedly improve mixing. This balloon atrial septostomy procedure is performed by passing a special balloon-tipped catheter into the heart from either a vessel in the umbilicus or a vessel in the groin. Often, the procedure is performed at the bedside, with guidance from an echocardiogram. Occasionally, the procedure will be performed in the catheterization laboratory.
A large atrial septal defect is therefore created and typically allows excellent mixing of oxygen-rich and oxygen-poor blood so that the body’s oxygen saturation will remain in a safe range, often in the 80 percent range. Following this procedure, the ductus arteriosus is no longer necessary and prostaglandin infusion can therefore be discontinued.
Although babies can be stabilized temporarily, surgical correction of the defect is always necessary. In most cases, corrective surgery is typically performed in the first week of life, once an infant has recovered from any instability that occurred during the initial presentation. In more complex cases, such as those with narrowing below the pulmonary valve (pulmonary stenosis), surgical timing is variable.
In most cases of transposition, an arterial switch operation is performed. The arterial switch operation involves cutting off the aorta and pulmonary arteries just above the point where they leave the heart, and reconnecting them to the proper ventricle. The valve stays attached to the ventricle, so what was once the pulmonary valve is now the aortic valve and vice versa.
Since the coronary arteries must stay with the aorta, they must be taken off the area above the valve and reimplanted separately above the new aortic valve. This is often the most technically challenging part of the operation, particularly if there is unusual branching of these arteries. Closure of ventricular septal defects (if present) and atrial septal defects is also performed as part of the operation.
Occasionally, in more complex cases of transposition such as in those narrowing below the pulmonary valve, the arterial switch operation is not recommended. These cases often involve complex decision making on a case-by-case basis to determine the best options and operative plan.1
References:
1https://www.cincinnatichildrens.org/health/t/transposition